A CASE OF 60 YEAR OLD MALE
Name: J. Akash
28/12/2022
Roll no. 53
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
Following is the view of my case :
Cheif complaints
A 60 year old male was brought to casuality with altered sensorium since yesterday night
History of presenting illness:
Patient was apparently asymptomatic 10 years back then he developed similar kind of symptom and was diagnosed with type 2 DM and started on OHA's later after few years (?3y) patient was shifted to Insulin (HAI twice daily)
After 4yrs Patient developed giddiness and while working patients had fall ,fracture Rt UL and Rt LL And diagnosed with HTN-( on anti hypertensive medication- Telma50 -ch12.5,METXL 40 )
2 yrs back patient developed similar episodes of altered sensorium and was having Hyperglycemia he went to pvt hospital at pvt hospital then was diagnosed to have? DKA → given Insulin and treated.
10 days back pt developed swelling of lower limb , and ulceration on right toe and Plantar aspect of foot for which he went to put practictiner and diagnosed to have diabetic foot and was treated with regular dressings and antibiotics.
From 4 days pt had nausea and vomitings (2 episodes per day) with food intake ,non blood tinged
vomitings not associated with fever ,cold ,cough,Pain abdomen, loose stools
Past history:
N/K/C/O asthma, CAD, Epilepsy
PERSONAL HISTORY
DIET MIXED
SLEEP ADEQUATE
BOWEL AND BLADDER MOVEMENTS REGULAR
ALCOHOL OCCASIONAL
NO SIGNIFICANT FAMILY HISTORY.
GENERAL EXAMINATION :
PT IS drowsy
NO PALOR, ICTERUS ,CYANOSIS,CLUBBING,EDEMA, LYMPHADENOPATHY
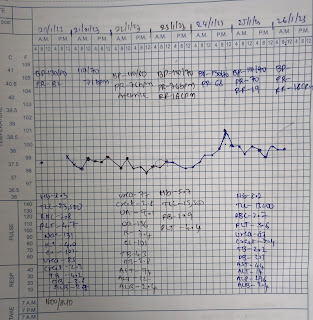
Vitals @ admission
Temp 98.6 F
Pr 86bpm
Bp 130/80mm hg
Spo2 97%
GRBS 123mg/dl
SYSTEMIC EXAMINATION:
CVS - S1,S2 +
RS - BAE + , NVBS
CNS - Pt is drowsy , arousable to deep pains
speech slurred
No meningial signs
GCS E3 V2 M5
Tone : RT LT
UL. N N
LT. N. N
REFLEXES: B. T. S. K. A. Plantar
RT. ++. ++. +. ++. + flexion
LT. +. + . +. + + flexion
INVESTIGATION:
CHEST XRAY :

USG -Abdomen

MRI - BRAIN

PROVISIONAL DIAGNOSIS:
)Altered sensorium secondary to hypotonic hyponatremia euvolemic ? SIADH
2)with small hemorraghic contusion of frontal lobe
3)With HTN since 4 years
4)with type2 DM
TREATMENT:
Given on 24/12/22
Iv fluids 3% Nacl @ 15ml/hr
RT feeds - 100 ml water 1 hrly 100 ml milk 2nd hrly
Inj.kcl 20 Meq in 100 ml NS over 2 hrs /IV / STAT
Inj Zofer 4 mg /Iv/Tid
Inj Pan 40 mg / Iv / Od
Inj. Hai sc tid acc to sliding scale
Syp. potchlor 15ml/po/Tid
ICU DAY2 25/12/22
AGE : 60Y GENDER :M
S:
No fever spikes
cough with sputum
O:
Pt is drowsy but arousable
oriented to person but not time and place
BP - 140/80 mm Hg
PR - 83 bpm
RR 21cpm
SPO2 - 98% @ RA
GRBS - 116 mg/dl
Temp - 98.4 F
CVS - S1,S2 +,Jvp not raised
RS - BAE + , NVBS
CNS - Pt is conscious but drowsy
No meningial signs
GCS E3 V4 M6
Tone : RT LT
UL N. N
LL N. N
REFLEXES: B. T. S. K. A. Plantar
RT. +. + . +. +. + flexion
LT. +. +. + + + flexion
A:
1)Altered sensorium secondary to hypotonic hyponatremia euvolemic ? SIADH
2)with small hemorraghic contusion of frontal lobe
3)With HTN since 4 years
4)with type2 DM
P:
Iv fluids 3% Nacl @ 15ml/hr( increase or decrease
acc to serum electrolytes
RT feeds - 100 ml water 1 hrly 100 ml milk 2nd hrly
(D1)Inj monocef 1g iv bd
Inj Zofer 4 mg /Iv sos
Inj Pan 40 mg / Iv / Od
Inj. Hai sc tid acc to sliding scale
(W/H)tab aldactone. 25 mg po bd
tab nicardia @10 mg po bd
coconut water through ryles tube 50ml bd
Syp. potchlor 15ml/po/Tid
26/12/22
UNIT 5
DR PRASUNA, INTERN
DR SANNITH, INTERN
DR HIMAJA, PGY1
DR DEEPIKA, PGY2
DR VINAY, PGY3
DR ABHINAYA, SR
ICU DAY 3
AGE : 60Y GENDER :M
S:
No fever spikes
O:
Pt is conscious
oriented to time and place and person
BP - 130/80 mm Hg
PR - 83 bpm
RR 17cpm
SPO2 - 98% @ RA
GRBS @8am 161
yesterday
8pm 129
10pm 145
2 am 117
8am 161
at 2pm 143 mg
Temp - 98.4 F
CVS - S1,S2 +,Jvp not raised
RS - BAE + , NVBS
p/a soft nontender
CNS - Pt is conscious
No meningial signs
GCS E4 V5 M6
Tone : RT LT
UL N. N
LL N. N
REFLEXES: B. T. S. K. A. Plantar
RT. +. + . +. +. - flexion
LT. +. +. + + -. flexion
power
UL. 5/5. 5/5
LL. 5/5. 5/5
A:
1)Altered sensorium secondary to hypotonic hyponatremia euvolemic ? SIADH
2)with small hemorraghic contusion of frontal lobe with AKI
3)With HTN since 4 years
4)with type2 DM since 18yrs
P:
Iv fluids 3% Ns @ 50ml/hr
RT feeds - 100 ml water 1 hrly 100 ml milk 2nd hrly
(D2)Inj monocef 1g iv bd
Inj Zofer 4 mg /Iv sos
Inj Pan 40 mg / Iv / Od
Inj. Hai sc tid acc to sliding scale
tab nicardia @10 mg po bd
coconut water through ryles tube 50ml bd
Syp. potchlor 15ml/po/Tid
tab TOLVAPTAN 15MG po od
27/12/22
UNIT 5
DR AKASH, INTERN
DR HYNDAVI, INTERN
DR HIMAJA, PGY1
DR DEEPIKA, PGY2
DR VINAY, PGY3
DR ABHINAYA, SR
ICU DAY 4
AGE : 60Y GENDER :M
S:
No fever spikes
O:
Pt is conscious , coherent,co operative
oriented to time and place and person
GCS- E4 V5 M6
BP - 160/90 mm Hg
PR - 92 bpm
RR 18cpm
SPO2 - 99%
GRBS @8am 199
Temp - 98.4 F
CVS - S1,S2 +,Jvp not raised
RS - BAE + , NVBS
P/A soft nontender
CNS - HMF intact
Tone : RT LT
UL N. N
LL N. N
REFLEXES: B. T. S. K. A. Plantar
RT. ++ + . +. +. + flexion
LT. ++ +. + + + flexion
power
UL. 5/5. 5/5
LL. 5/5. 5/5
A:
1)Altered sensorium secondary to hypotonic hyponatremia euvolemic ? SIADH
2)with small hemorraghic contusion of frontal lobe with AKI
3)With HTN since 4 years
4)with type2 DM since 18yrs
P:
Iv fluids Ns @ 50ml/hr
RT feeds - 100 ml water 1 hrly 100 ml milk 2nd hrly
(D3)Inj monocef 1g iv bd
Inj Zofer 4 mg /Iv sos
Inj. Hai sc tid acc to sliding scale
tab nicardia @10 mg po bd
Syp. POTCHLOR 15ml/RT/Tid
tab TOLVAPTAN 15MG po od
28/12/22
UNIT 5
DR HIMAJA, PGY1
DR DEEPIKA, PGY2
DR VINAY, PGY3
DR ABHINAYA, SR
DR AKASH, INTERN
DR HYNDAVI, INTERN
AMC, DAY 5
AGE : 60Y GENDER :M
S:
No fever spikes
O:
Pt is conscious , coherent,co operative
oriented to time and place and person
GCS- E4 V5 M6
BP - 130/90 mm Hg
PR - 96 bpm
RR 16cpm
SPO2 - 98%
GRBS @8am 224
Temp - 98F
CVS - S1,S2 +,Jvp not raised
RS - BAE + , NVBS
P/A soft nontender
CNS - HMF intact
Tone : RT LT
UL N. N
LL N. N
REFLEXES: B. T. S. K. A. Plantar
RT. + + . + +. + flexion
LT. + + + + + flexion
power
UL. 5/5. 5/5
LL. 5/5. 5/5
A:
1.Altered sensorium secondary to hyponatremia euvolemic ? SIADH?
2)with small hemorraghic contusion of frontal lobe with AKI(resolving)
3)With HTN since 4 years
4)with type2 DM since 18yrs
P:
Iv fluids Ns @ 50ml/hr
RT feeds - 100 ml water 1 hrly 100 ml milk 2nd
(D4)Inj monocef 1g iv bd
Inj Zofer 4 mg /Iv sos
Inj. Hai sc tid acc to sliding scale
tab nicardia @10 mg po bd
Syp. POTCHLOR 15ml/RT/Tid
tab TOLVAPTAN 15MG po /od

Comments
Post a Comment