65 year old female with Generalised weakness
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients’ clinical problems with collective current best evidence-based inputs.
J. Akash
R.no. 43
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
A 65 year old female came to the hospital with the chief complaint of :
Generalised weakness since 3 months
pain and burning sensation in the fingertips since 2months
Difficulty in swallowing since 2 months &Hoarseness of voice since 5days
Ear pain since 2 months
HISTORY OF PRESENTING ILLNESS :
patient was apparently normal 3 years back then she was diagnosed with Diabetes & she is on oral hypoglycemic drugs
History of Generalised weakness since 1 year
History of difficulty in swallowing to solids , normal to fluids.for dysphagia she was given some antibiotics and analgesics by local doctor
History of ear pain which was aggrevating on exposure to air, reliving on taking medication not associated with any discharge
She developed Pain & burning Sensation in the distal finger tips which was aggrevating while eating & relieving on taking medication
she came to hospital with the same complaints on 28th march 2022 ,she was prescribed medication & advised to admit hospital.
She history of fall on 28th march in the evng when she went to take bath.
Due to trauma hematoma is formed around eye

PERSONAL HISTORY:
Appetite: Normal
Diet: mixed
Bowel& bladder: regular
Sleep: adequate
Addictions: No addictions
PAST HISTORY:
She has deviation of mouth since age of 5months on right side , she was on herbal medication
-She is a known case of diabetes mellitus since 3 years and she is on regular medication.
MENSTRUAL HISTORY: attained menopause
FAMILY HISTORY : Insignificant
GENERAL EXAMINATION:
Patient is conscious, coherent and co-operative; well oriented to time, person, place.
Well built and well nourished.


No pallor ,icterus, clubbing, cyanosis, edema, generalised lymphadenopathy.
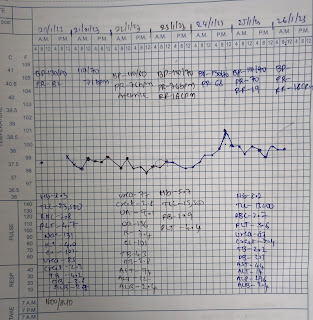
Vitals :
Temperature: Afebrile
Pulse : 82bpm
BP : 100/70 mm of Hg
RR: 17 cpm
SYSTEMIC EXAMINATION:
CNS :
highmotor function: intact
Tone: Right Left
upperlimb Normal normal
lowelimb : normal normal
Power: Right left
upperlimb 5/5. 5/5
lowerlimb 5/5 5/5
INVESTIGATIONS:
RBS: 164 mg/dl
Se. Creatinine: 1.2 mg/dL( on 29/3/2022)
2.4mg /dL ( on 28/3/2022)
Se. Uric acid: 11.1 mg/dL
Blood urea: 41 mg/dL
Na: 138 mEq/L
K: 4.8 mEq/L
Cl: 101 mEq/L
LFT:
Db: 0.16 mg/dL
Tb: 0.57 mg/dL
AST: 64 IU/L
ALT: 57 IU/L
ALP: 204 IU/L
TP: 8.0 gm/dL
Albumin: 3.6 g/dL
A/G ratio: 0.89
Chest X-ray:

ECG:

Xrays:



Provisional Diagnosis:
Reynauds phenomenon with? scleroderma(sclerodactyly)
With laryngopharyngeal reflux disease with
Right mild NPDR & Left moderate NPDR
Treatment :
1. Tab. NIFEDIPINE 10mg TID
2. IV FLUIDS 2 NS
3. Inj. ACTRAPID 10 units
(Morning- afternoon-night)
4. Tab. FOLITRAX ( methotrexate)7.5mg once a week
Every Wednesday
5. Tab.FOLIC ACID 5mg once a week on Tuesday
Treatment plan on 01/04/2022 :


Comments
Post a Comment